How we ship hospital management systems for 250-bed hospitals.
The pattern Xenara uses to deploy HMS at 250-bed multi-specialty hospitals — operational discovery, phased rollout, billing engine architecture, compliance baked in, and the change management that decides whether the system gets adopted. Live example: Asian Institute of Medical Sciences (AIMS) Hyderabad.
- Bed range
- 150 – 400
- Rollout pattern
- 5 phases
- OPD pilot
- 8 – 10 wks
- Full deployment
- 6 – 9 mo
Multi-specialty hospitals where this archetype fits.
Discovery → foundation → modules → go-live → steady state.
First department live with billing core.
All modules across 250+ beds, phased.
Last updated
Who this archetype is for
Multi-specialty hospitals in the 150–400 bed range with active OPD volumes, IPD operations, in-house lab and pharmacy, multi-tier billing, and accreditation (NABH, NABL, JCI, ISO 15189) on the radar or in hand. The playbook is the same whether the hospital is in Pakistan, India, the UAE, or another emerging market — local billing rails, language, and connectivity profile change the configuration, not the architecture.
Why off-the-shelf HMS rarely works at this scale
- Multi-tier OPD billing (self-pay / panel / insurer / corporate) treated as exception not native flow.
- Local payment rails (JazzCash, Easypaisa, 1Link, NIFT, UPI) bolted on as workarounds.
- Audit logging retrofitted, not designed in — slows accreditation cycles.
- Print stack assumes Latin script — Urdu / Hindi / Arabic typography needs custom work anyway.
- Connectivity assumptions don't match Pakistani / South Asian / Middle East infrastructure reality.
The Xenara archetype
1. Operational discovery (2–3 weeks)
Engineers walk every department before scoping. OPD registration on a peak day. IPD ward operations across shifts. Lab order-to-result cycle. Pharmacy dispensing flow. End-of-day cash reconciliation. The HMS is designed against the operation observed — not a feature list.
Output: written discovery document with department-by-department workflow, integration surface, compliance targets, and a phased delivery plan with milestones and a fixed price for the build phase.
2. Foundation build (weeks 4–8)
- Patient master with demographics, identifiers, history, family linkages, photo-on-file.
- User and role management — clerks, nurses, doctors, lab techs, pharmacists, billing, administration.
- Audit logging baked into every PHI-touching action from day one.
- Billing engine: multi-tier pricing, panel routing, hybrid sales (card + cash + wallet), refunds.
- First end-to-end OPD slice live in staging.
3. Module rollout (OPD first)
Pilot one department — almost always OPD because volume and operational friction are highest there. OPD goes live with the new HMS while paper runs in parallel for 1–2 weeks. Once OPD is stable, IPD comes next. Then lab. Then pharmacy. Then operational reporting. Modules layer onto the same patient master and billing engine.
4. Go-live + training
Phased go-live, on-site Xenara engineers during the first weekends, in-person training at the counter (not in a classroom). Clerks teach the next shift by day three. On-call coverage for 30 days after each phase launches.
5. Steady state + evolution
Monthly retainer for bug fixes, new modules, integrations, regulatory changes. Same engineers who built it stay on the work.
Architecture decisions that matter
- On-prem or hybrid hosting: Database on hospital servers, application server on-prem or in a controlled cloud region. Decided per board / accreditor preference.
- Audit log: Append-only, signed, exportable on demand. NABH/NABL/JCI auditors expect to see who-saw-what within minutes, not days.
- Print stack: Multilingual rendering — Noto Nastaliq Urdu, Devanagari for Hindi, Arabic with RTL where required.
- Connectivity resilience: Local cache + sync queue. Front-desk and lab keep operating through outages; sync resumes on reconnect.
- Integration surface: HL7 v2 / FHIR for EMR interoperability, file-drop or proprietary REST for lab analyzers, accounting integration for billing reconciliation.
Compliance the audit team can read
- Role-based access scoped to functional duties, reviewable per user per role.
- Encryption at rest and in transit.
- Audit log exportable per patient, per user, per action type.
- Configurable data residency — chosen per deployment based on regulator / accreditor / board policy.
Indicative cost bands
Directional only — actual pricing depends on bed count, integration scope, on-prem vs cloud, and SLA. Shared so finance and procurement can sanity-check whether custom HMS belongs in the conversation before discovery starts.
| Engagement scope | Pakistan (PKR) | Canada / US (CAD) | Timeline |
|---|---|---|---|
| Phase 1 — OPD pilot + foundation | PKR 12M – 22M | CAD 80,000 – 150,000 | 8 – 12 weeks |
| Phase 2 — IPD + lab + pharmacy + billing | PKR 18M – 35M | CAD 120,000 – 240,000 | 10 – 16 weeks |
| Full deployment (250 beds, all modules, on-prem + DR) | PKR 35M – 70M+ | CAD 230,000 – 500,000+ | 6 – 9 months phased |
| Ongoing — hosting, support, on-call, evolution | PKR 6M – 14M / yr | CAD 40,000 – 95,000 / yr | 12 / 24-month retainer |
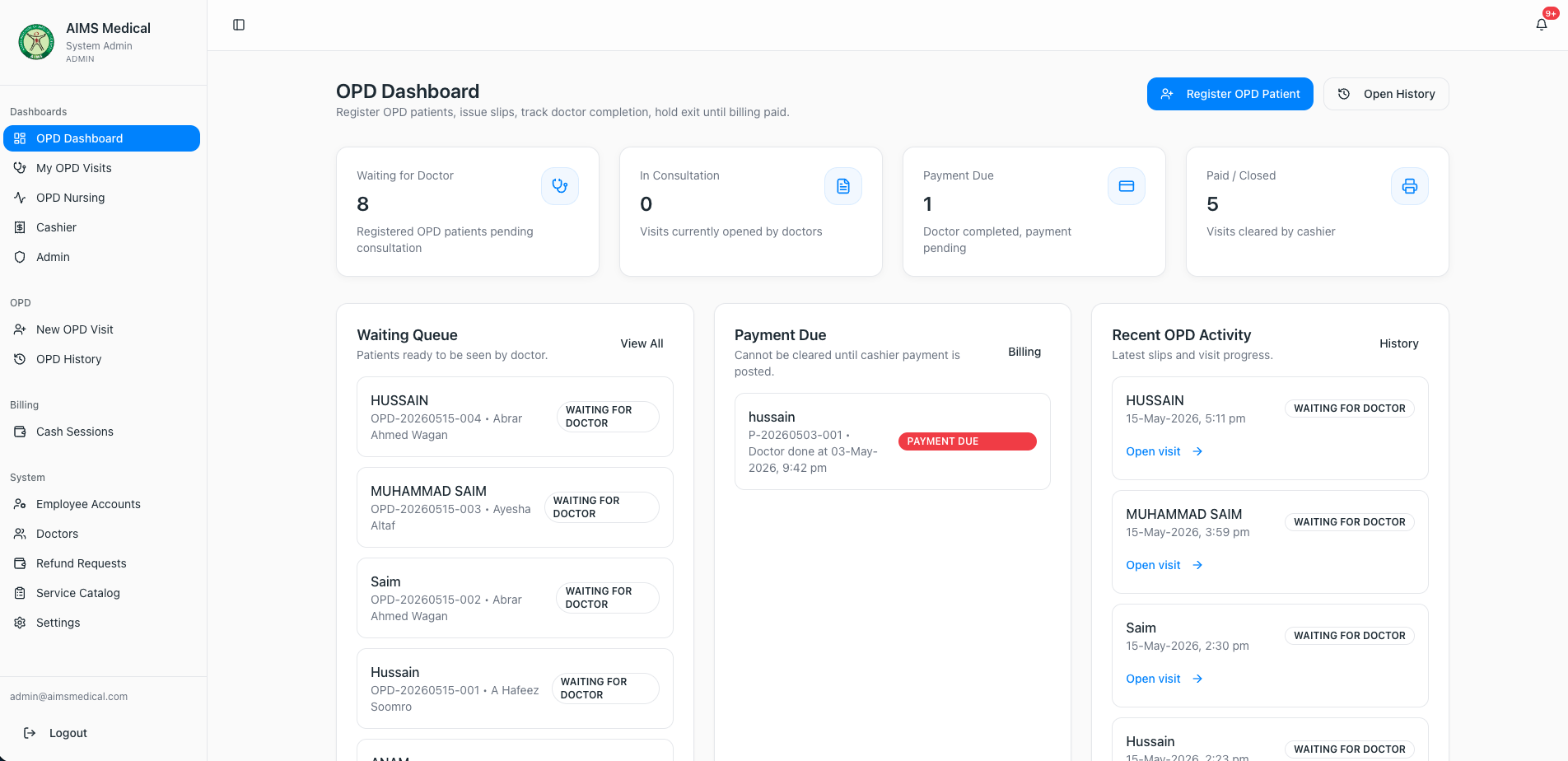
Live example: AIMS Hyderabad
Asian Institute of Medical Sciences — 250-bed NABH-accredited super-specialty hospital
Custom HMS live across OPD, IPD, lab, pharmacy, and billing in Sindh, Pakistan. Operational reporting previously taking days now runs in minutes.
Read the AIMS case studyIf you're evaluating an HMS
Talk to Xenara before signing with any vendor. We'll walk your operation, map your real workflows, and give an honest assessment of whether custom HMS or off-the-shelf is the right call. See our HMS development service or email hello@xenara.ai.